

*Editor’s Note: elephant journal articles represent the personal views of the authors, and can not possibly reflect elephant journal as a whole. Disagree with an Op-Ed or opinion? We’re happy to share your experience here. This website is not designed to, and should not be construed to, provide medical advice, professional diagnosis, opinion or treatment to you or any other individual, and is not intended as a substitute for medical or professional care and treatment. For serious.
~
Why Current Thinking about Autism is Completely Wrong
Autism rates have skyrocketed. Today an estimated one in 150 kids today has been diagnosed.
Over the past 10 to 20 years, dramatic scientific discoveries have turned conventional thinking about autism on its head. For example, Martha Herbert, MD, a pediatric neurologist from Harvard Medical School, showed how core abnormalities in immunity, gut function, and detoxification play a central role in causing autism’s behavioral and mood symptoms.
Dr. Herbert argues everything is connected. That these kids have smelly bowel movements, bloated bellies, frequent colds and ear infections, and dry skin is no coincidence. Unfortunately, conventional medicine often ignores this central point about why these kids become sick.
Sam’s story provides some clues about why autism is a systemic disorder rather than a genetic brain disorder.
Sam’s mother desperately came to see me because her son, who was two and a half at the time, had just been diagnosed with autism. He was born bright and happy, breastfed, with the best medical care available including all the vaccinations he could possibly have. He talked, walked, loved, and played normally.
All that occurred until 22 months, after which Sam had measles, mumps, and rubella vaccinations. Something changed around that time.
Vaccines affect susceptible children through different mechanisms. In some, they overwhelm an already-taxed immune system. For other kids, thimerosal (ethylmercury) used as a preservative until recently in most vaccines (although it is still present in most flu vaccines) creates problems.
In Sam’s situation, he lost his language abilities and became detached, less interactive, and unable to relate with others.
Based on these symptoms, doctors “pronounced” Sam as having autism, as if it were a thing you catch like a bug. They claimed nothing could be done except arduously painful and barely effective behavioral and occupational therapy techniques. Progress would be slow, and his parents should keep their expectations low.
Devastated, his mother began to seek other options and found her way to me.
While uncovering underlying causes isn’t always easy, treating autism as a body disorder that affects the brain gives us so many other treatment choices. Children treated in this way often have dramatic and remarkable—if not miraculous—recoveries.
Biochemical individuality underlies functional medicine. If you take 100 kids with autism, each one may have unique genetics, causes, and triggers that require very different treatments to become better.
Autism is just a label. Like every condition or illness, we must uncover what is really happening. Rather than one thing, usually a collection of insults, toxins, and deficiencies piled on susceptible genetics leads to biochemical train wreaks we see in these children.
When I first saw him, Sam was deep in the inner wordless world of autism. Watching him was like watching someone on a psychedelic drug trip. We dug into his biochemistry and genetics to find several things that accounted for his problems. Among them:
- He had very high level of antibodies to gluten. He had allergies to about 28 foods, including wheat, dairy, eggs, yeast, and soy,
- He had a leaky gut that showed a high level of an inflammatory marker called eosinophil protein X. He had three species of yeast growing in his gut and no growth of healthy bacteria. Urine tests showed very high levels of D-lactate, an indicator of overgrowth of bacteria in the small intestine.
- He had nutrient deficiencies.
- His amino acids—necessary for normal brain function and detoxification—were depleted.
- His blood showed high levels of aluminum and lead, while his hair showed very high levels of antimony and arsenic, signs of a very toxic little boy.
- His sulfur and glutathione levels were low, indicating he just couldn’t muster the power to detox all these metals. In fact, his genes showed a major weak spot in glutathione metabolism, which is the body’s main antioxidant and major detoxification highway for getting rid of metals and pesticides.
- He had trouble with a key biochemical function called methylation required to make normal neurotransmitters and brain chemicals and critical for helping the body rid toxins. This showed up as low levels of homocysteine (signs of problems with folate metabolism) and high methylmalonic acid (signs of problems with B12 metabolism). He also had two genes that set him up for more problems with this system.
- He had very high levels of oxidative stress or free radical activity, including markers that told me his brain was inflamed and under free-radical fire.
As with every patient, I designed a plan to help Sam address these issues. In functional medicine, we remove what causes the problems and, based on biochemical uniqueness, provide what the individual requires to thrive. Then the body does the rest.
Here is the roadmap I used to help Sam recover. In this order, we:
- Fixed the gut and reduced inflammation. That included eliminating gluten and other food allergens, providing anti-fungals to reduce yeast, using antibiotics to destroy small intestinal toxic bacteria, replenishing healthy bacteria with probiotics, and digestive enzymes to break down food.
- Replenished nutrients. Those included zinc, magnesium, folate, and vitamins A, B6, B12, and D as well as omega-3 fats.
- Detoxified and reduced oxidative stress.
We saw some dramatic improvements that became even better over time:
- After following a gluten-free diet and treating his gut for three weeks, Sam showed dramatic and remarkable improvement. Most of his language skills returned and he seemed much more connected and interactive with others.
- After four months, he was more focused, unstuck, and verbal.
- After 10 months, his bowels were back to normal, he was verbally fluent, mainstreamed in school, and he “lost” his diagnosis of autism.
- After two years all his abnormal tests were normal including the high metals, gut inflammation, and damage to his mitochondria and free radicals.
Not every child has such a dramatic recovery but many improve, and some improve dramatically using the approach of functional or systems medicine.
Have you or anyone you know taken a whole-body approach to autism or any other medical diagnosis? Share your results below or on my Facebook fan page.
~
References
Because of the interest in this topic and controversies surrounding it, I am posting all the references for the issues talked about in the article.
- Curtis TR, ed. The London Encyclopedia. London: Griffi n and Co; 1839.
- James SJ, Melnyk S, Jernigan S, et al. Metabolic endophenotype and related genotypes are associated with oxidative stress in children with autism. Am J Med Genet B Neuropsychiatr Genet. 2006;141B(8):947-956.
- Williams TA, Mars AE, Buyske SG, et al. Risk of autistic disorder in affected offspring of mothers with a glutathione S-transferase P1 haplotype. Arch Pediatr Adolesc Med. 2007;161(4):356-361.
- Reddy MN. Reference ranges for total homocysteine in children. Clin Chim Acta. 1997;262(1-2):153-155.
- James SJ, Cutler P, Melnyk S, et al. Metabolic biomarkers of increased oxidative stress and impaired methylation capacity in children with autism. Am J Clin Nutr. 2004;80(6):1611-1617.
- Bull G, Shattock P, Whiteley P, et al. Indolyl-3-acryloylglycine (IAG) is a putative diagnostic urinary marker for autism spectrum disorders. Med Sci Monit. 2003;9(10):CR422-CR425.
- Wright B, Brzozowski AM, Calvert E, et al. Is the presence of urinary indolyl-3-acryloylglycine associated with autism spectrum disorder? Dev Med Child Neurol. 2005;47(3):190-192.
- Amminger GP, Berger GE, Schäfer MR, Klier C, Friedrich MH, Feucht M. Omega-3 fatty acids supplementation in children with autism: a double-blind randomized, placebo- controlled pilot study. Biol Psychiatry. 2007;61(4):551-553.
- Johnson SM, Hollander E. Evidence that eicosapentaenoic acid is effective in treating autism. J Clin Psychiatry. 2003;64(7):848-849.
- Poling JS, Frye RE, Shoffner J, Zimmerman AW. Developmental regression and mitochondrial dysfunction in a child with autism. J Child Neurol. 2006;21(2):170-172.
- Herbert MR. Autism: A brain disorder or a disorder of the brain? Clin Neuropsychiatry. 2005;2(6):354-379.
- Herbert MR. Large brains in autism: the challenge of pervasive abnormality. Neuroscientist. 2005;11(5):417-440.
- Vargas DL, Nascimbene C, Krishnan C, Zimmerman AW, Pardo CA. Neuroglial activation and neuroinflammation in the brain of patients with autism. Ann Neurol. 2005;57(1):67-81. Erratum in: Ann Neurol. 2005 Feb;57(2):304.
- Wakefi eld AJ, Ashwood P, Limb K, Anthony A. The signifi cance of ileo-colonic lymphoid nodular hyperplasia in children with autistic spectrum disorder. Eur J Gastroenterol Hepatol. 2005;17(8):827-836.
- Millward C, Ferriter M, Calver S, Connell-Jones G. Gluten- and casein-free diets for autistic spectrum disorder. Cochrane Database Syst Rev. 2004;(2):CD003498.
- Uhlmann V, Martin CM, Sheils O, et al. Potential viral pathogenic mechanism for new variant infl ammatory bowel disease. Mol Pathol. 2002;55(2):84-90.
- Kawashima H, Mori T, Kashiwagi Y, Takekuma K, Hoshika A, Wakefi eld A. Detection and sequencing of measles virus from peripheral mononuclear cells from patients with inflammatory bowel disease and autism. Dig Dis Sci. 2000;45(4):723-729.
- Hornig M, Briese T, Buie T, et al. Lack of association between measles virus vaccine and autism with enteropathy: a case-control study. PLoS ONE. 2008;3(9):e3140.
- Bradstreet JJ, El Dahr J, Anthony A, Kartzinel JJ, Wakefi eld AJ. Detection of measles virus genomic RNA in cerebrospinal fl uid of children with regressive autism: a report of three cases. J Am Phys Surgeons. 2004;9(2):38-45.
- Taylor B, Miller E, Farrington CP, et al. Autism and measles, mumps, and rubella vaccine: no epidemiological evidence for a causal association. Lancet. 1999;353(9169):2026-2029.
- Williams R. Biochemical Individuality, New York: McGraw Hill; 1998.
- Autism Research Initiative. Treatment Options for Mercury/metal Toxicity in Autism and Related Developmental Disabilities: Consensus Position Paper. San Diego, CA: Autism Research Initiative; 2005. Available at: http://www.autism.com heavymetals.pdf. Accessed September 17, 2008.
- Holmes AS, Blaxill MF, Haley BE. Reduced levels of mercury in fi rst baby haircuts of autistic children. Int J Toxicol. 2003;22(4):277-285.
- Adams JB, Romdalvik J, Ramanujam VM, Legator MS. Mercury, lead, and zinc in baby teeth of children with autism versus controls. J Toxicol Environ Health A. 2007;70(12):1046-1051.
- Thompson WW, Price C, Goodson B, et al. Early thimerosal exposure and neuropsychological outcomes at 7 to 10 years. N Engl J Med. 2007;357(13):1281-1292.
- Geier DA, Geier MR. A prospective study of mercury toxicity biomarkers in autistic spectrum disorders. J Toxicol Environ Health A. 2007;70(20):1723-1730.
- Echeverria D, Woods JS, Heyer NJ, et al. The association between a genetic polymorphism of coproporphyrinogen oxidase, dental mercury exposure and neurobehavioral response in humans. Neurotoxicol Teratol. 2006;28(1):39-48
- Heyer NJ, Echeverria D, Bittner AC Jr, Farin FM, Garabedian CC, Woods JS. Chronic low-level mercury exposure, BDNF polymorphism, and associations with self-reported symptoms and mood. Toxicol Sci. 2004;81(2):354-363. Epub 2004 Jul 14.
- Echeverria D, Woods JS, Heyer NJ, et al. Chronic low-level mercury exposure, BDNF polymorphism, and associations with cognitive and motor function. Neurotoxicol Teratol. 2005;27(6):781-796.
~
~
Love elephant and want to go steady?
Sign up for our (curated) daily and weekly newsletters!
Author: Dr. Mark Hyman
Editor: Rachel Nussbaum
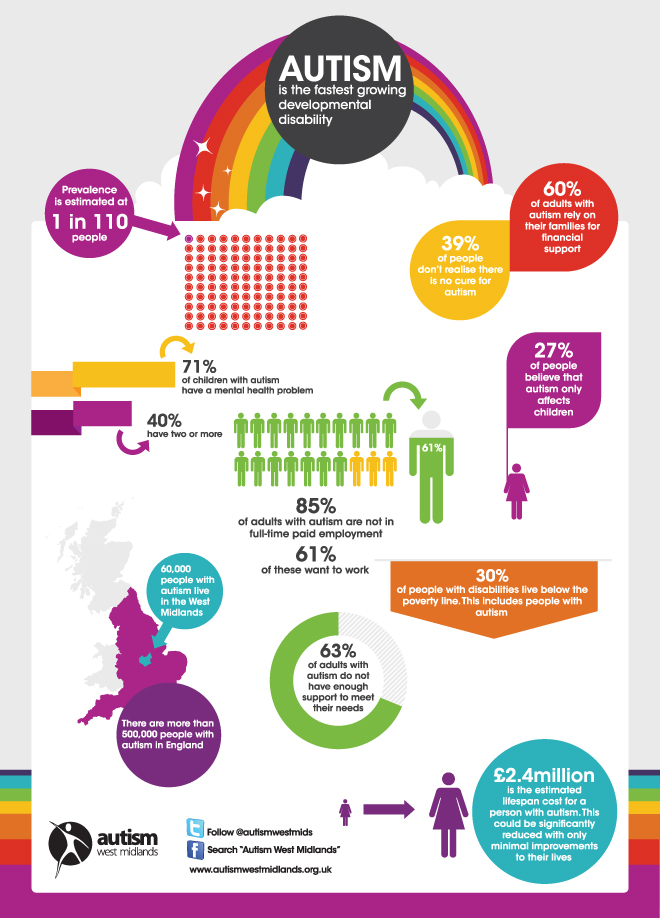
Photo: Autism West Midlands




Read 0 comments and reply